The group coordinator should register and launch the webinar using instructions from the email confirmation. Each participant will process their own CE online.
If the webinar exceeds maximum capacity, you may be unable to connect. Please feel free to access the audio using the phone number provided in your webinar confirmation email and follow along with the handout.
A comprehensive handout with speaker information, PPT slides, and references will be available for download approximately 24 hours prior to the activity. Onsite attendees will be provided with a printed handout.
The Webinar and Midyear symposium will be developed into an online CE activity (audio synched with PPT slides). Participants should claim CE credit for this home-study educational activity only if they have not claimed credit for the live activity.
Contact elearning@ashp.org for questions and assistance related to this activity.
Clinical Updates
Focusing on Prevention, Treatment and Recurrence of Clostridium Difficile Infection
ASHP Advantage e-Newsletter
Management Challenges and New and Emerging Therapeutic Modalities
ASHP Advantage e-Newsletter
Spring 2019
Introduction
Infections caused by Clostridioides difficile (C. difficile), a spore-forming, Gram-positive anaerobic bacillus also known as Clostridium difficile, are a major health threat in the United States. The pathogen produces two exotoxins (toxin A and toxin B) that can cause local gastrointestinal (GI) mucosal damage and systemic effects. Recurrence of C. difficile infection (CDI) is common, affecting approximately one in four or five patients. Severe fulminant colitis and potentially fatal toxic megacolon can develop. Infections caused by C. difficile affect more than 450,000 Americans and cause more than 29,000 deaths annually, with an estimated cost of $1.5 billion.
ASHP Advantage is conducting an educational initiative on the management of CDI for physicians, pharmacists, physician assistants, and nurse practitioners. Two free on-demand continuing education activities featuring the faculty team of Kevin W. Garey, Pharm.D., M.S., FASHP, and Krishna Rao, M.D., M.S., are available on the initiative website. Dr. Garey is Professor at the University of Houston College of Pharmacy and Chair of the Department of Clinical Sciences and Administration at the University of Houston College of Pharmacy in Houston. Dr. Rao is Assistant Professor of Internal Medicine at the University of Michigan in Ann Arbor.
In the first activity, Drs. Garey and Rao provide an overview of best practices for CDI management, including an update on clinical practice guidelines and stewardship strategies. They then build on that foundation during the second activity by illustrating the application of the CDI guidelines to patient cases and describing the role of new and emerging therapies for CDI.
This e-newsletter provides updates on these programs and addresses challenges in managing patients with CDI.
Initiative Faculty
Kevin W. Garey, Pharm.D., M.S., FASHP
Professor and Chair
Department of Clinical Sciences and Administration
University of Houston College of Pharmacy
Houston, Texas View Bio
Krishna Rao, M.D., M.S.
Assistant Professor of Internal Medicine
University of Michigan
Ann Arbor, Michigan View Bio
Testing for CDI
Managing CDI poses a challenge to clinicians because of uncertainty, unresolved controversy, and the ongoing emergence of new data about the optimal therapeutic strategy. Questions sometimes arise about which patients should be tested for CDI. Clinicians should have a high index of suspicion about the possibility of CDI in patients with certain symptoms (Table). Testing for CDI should not be performed for asymptomatic patients because colonization is common, especially among certain groups (e.g., 60% to 70% of infants, 20% to 50% of adults in long-term care facilities). Positive test results may reflect colonization without infection. Treatment is not indicated for asymptomatic patients because it typically does not affect the risk, epidemiology, or transmission of CDI.
Testing for CDI should not be performed during or immediately after treatment for the infection because the results can be misleading. Positive test results do not necessarily reflect treatment failure. Up to half of patients have positive test results 6 weeks after the completion of treatment because of the shedding of spores. Approximately 10% to 20% of patients treated for CDI become long-term carriers, and treatment of carriers is controversial because of an apparent lack of benefit. Repeat testing for cure after treatment is not recommended unless a patient is symptomatic.
Table. Indications for Testing for CDI
Diarrhea (defined as three or more loose bowel movements in a 24-hour period without an identifiable cause, such as receipt of contrast media or recent initiation of tube feedings)
Ileus with leukocytosis
Colitis on imaging
Acute abdomen with bowel wall thickening
Toxic megacolon
Pseudomembranes on endoscopy
Post-infectious irritable bowel syndrome (IBS) is common after treatment for and recovery from CDI. It is attributed to long-term colonization with C. difficile and can be difficult to differentiate from recurrent CDI. Post-infectious IBS usually manifests as milder illness compared with the initial CDI episode, and testing for recurrent CDI is unnecessary in patients with this presentation.
Patients with inflammatory bowel disease (IBD) have higher rates of C. difficile carriage (i.e., colonization) than the general population. Diagnosing and treating CDI in these patients pose unique challenges because CDI can mimic or trigger an IBD flare (there is overlap in symptoms). There is a lack of consensus among gastroenterologists about whether to use antibiotics alone or in combination with immunomodulators (e.g., corticosteroids) to treat CDI, flares, or both in patients with IBD and CDI. In a retrospective analysis by Ben-Horin and colleagues of hospitalized patients with IBD and CDI who were treated with antibiotics with or without immunomodulators, combination therapy was associated with worse outcomes than antibiotic therapy alone. A possible approach to managing patients with IBD who present with symptoms that suggest CDI (i.e., diarrhea) is to perform a stool test for toxigenic C. difficile and start treatment for CDI if it is present (Figure 1). Immunosuppressive therapy would be started or escalated if C. difficile is not present in the stool or if CDI symptoms do not improve after 48 hours of treatment for CDI.
Testing for CDI should be performed using only an unformed stool sample from patients with diarrhea. Various assays are available that detect or measure the organism, the toxins that it produces, and/or its genes.
What’s in a Name?
In 2018 the Clinical & Laboratory Standards Institute reclassified and renamed Clostridium difficile as Clostridioides difficile. This nomenclature change will be reflected in 2019 documents from the Centers for Disease Control and Prevention and others. The old name Clostridium difficile remains valid and can still be used, although the newer name is now preferred in publications.
More Information
Lawson PA, Citron DM, Tyrrell KL, Finegold SM. Reclassification of Clostridium difficile as Clostridioides difficile (Hall and O'Toole 1935) Prévot 1938. Anaerobe. 2016; 40:95-9.
Tindall BJ. Misunderstanding the Bacteriological Code. Int J Syst Bacteriol. 1999; 49(Pt 3):1313-6.
Figure 1. Suggested Algorithm for Managing Patients with IBD Presenting with Symptoms Consistent with CDI
(a)Abbreviations: CDI, Clostridium difficile infection; IBD, inflammatory bowel disease.
(b)Rao K, Higgins PD, Epidemiology, Diagnosis, and Management of Clostridium difficile Infection in Patients with Inflammatory Bowel Disease, Inflamm Bowel Dis, 2016, 22(7), page 22, by permission of Oxford University Press.
Which of the following enzyme immunoassay (EIA) methods is most appropriate to use to test for CDI?
A Glutamate dehydrogenase (GDH) EIA alone
B Glutamate dehydrogenase (GDH) EIA with toxin EIA
C Toxin EIA alone
Explanation Glutamate dehydrogenase (GDH) enzyme immunoassay (EIA) is used to detect C. difficile, which secretes the enzyme, but GDH EIA typically is paired with toxin EIA because GDH EIA detects both toxigenic and nontoxigenic C. difficile strains. Use of GDH EIA alone is not sufficient. Polymerase chain reaction (PCR) testing for the toxin B gene is an alternative to use of GDH EIA plus toxin EIA. Use of toxin EIA alone is not recommended because of a lack of sensitivity.
Nucleic acid amplification testing, which uses PCR technology, can be used to detect toxigenic C. difficile with high sensitivity and specificity for the presence of the organism, although it does not detect the toxin. Therefore, this PCR test is potentially less specific for C. difficile infection and may instead reflect colonization, although the differential diagnosis might be made by taking into consideration the patient presentation (i.e., symptoms).
More Information
Bagdasarian N, Rao K, Malani PN. Diagnosis and treatment of Clostridium difficile in adults: a systematic review. JAMA. 2015; 313:398-408.
Ben-Horin S, Margalit M, Bossuyt P et al. Combination immunomodulator and antibiotic treatment in patients with inflammatory bowel disease and Clostridium difficile infection. Clin Gastroenterol Hepatol. 2009; 7:981-7.
Rao K, Higgins PD. Epidemiology, diagnosis, and management of Clostridium difficile infection in patients with inflammatory bowel disease. Inflamm Bowel Dis. 2016; 22:1744-54. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4911291/pdf/nihms767050.pdf.
Brecher SM, Novak-Weekley SM, Nagy E. Laboratory diagnosis of Clostridium difficile infections: there is light at the end of the colon. Clin Infect Dis. 2013; 57:1175-81.
Prolonged, Tapered, and Pulsed Therapy
The goals of treatment for CDI include correcting dysbiosis (i.e., restoring the indigenous microbiota), killing the pathogen, and if possible, modifying the adaptive immune response that causes damage to the GI mucosa and systemic effects. Metronidazole is no longer recommended for initial episodes in treatment guidelines for CDI from the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA) because of its inferior clinical success and higher 30-day mortality compared with vancomycin. In current IDSA/SHEA guidelines, fidaxomicin (a narrow-spectrum, non-absorbable antibiotic) is an alternative to vancomycin because of its noninferior efficacy and the significantly lower risk of CDI recurrence compared with vancomycin. Metronidazole is reserved for use if vancomycin and fidaxomicin are not available or not tolerated.
Treating and preventing CDI recurrence can present a challenge to clinicians, especially for patients with multiple recurrences. Switching to an antibiotic that was not used to treat the initial episode is an intuitive approach that is recommended for a first recurrence. Use of a prolonged, tapered, and pulsed vancomycin regimen (125 mg orally four times daily for days 10-14, followed by two times daily for 1 week, once daily for 1 week, and once every 2 or 3 days for 2-8 weeks instead of the standard 125 mg orally four times daily for 10 days) is an option for treating first recurrences if standard vancomycin was used for treatment of the initial episode. A prolonged, tapered, and pulsed vancomycin regimen also is an option for the treatment of second and subsequent recurrences.
In theory, providing prolonged and progressively lower antibiotic exposure allows more time for clearance of C. difficile, and the antibiotic-free periods during pulsed (i.e., intermittent) administration allow replenishment of the normal microbiota. In a small study of 100 patients with recurrent CDI in whom vancomycin administration had been tapered, the use of pulsed vancomycin doses every 3 days instead of every 2 days substantially increased the clinical cure rate from 61% to 81%. This change in pulse therapy frequency increased the total duration of vancomycin therapy by nearly 50%.
The use of prolonged and pulsed fidaxomicin without a taper (200 mg orally twice daily on days 1-5 followed by once daily every other day on days 7-25) instead of the standard vancomycin regimen (125 mg orally four times daily on days 1-10) was shown to significantly reduce the rate of CDI recurrence in 356 patients 60 years of age or older with initial or recurrent CDI in the EXTEND trial. This prolonged, pulsed fidaxomicin regimen is not recommended in current IDSA/SHEA treatment guidelines.
“Chaser” Therapy
The use of “chaser” or “follow-on” rifaximin, which is a non-absorbable rifamycin antibiotic approved by the Food and Drug Administration for the treatment of traveler’s diarrhea, for preventing CDI recurrence has been explored after resolution of CDI using primary treatment. In a study of 130 patients with resolution of CDI using vancomycin or metronidazole, a significant reduction in the rate of CDI recurrence within 12 weeks was associated with the use of rifaximin 400 mg three times a day for 2 weeks, followed by 200 mg three times a day for another 2 weeks instead of placebo (16% vs. 30%, respectively, p = 0.06). Current IDSA/SHEA treatment guidelines include the use of rifaximin 400 mg orally three times daily for 20 days as a chaser after 10 days of vancomycin 125 mg orally four times daily as an option for treating patients with a second or subsequent CDI recurrence. Resistance develops rapidly to rifaximin, so the use of fidaxomicin in place of rifaximin as chaser therapy after vancomycin has been investigated.
More Information
Gentry CA, Giancola SE, Thind S et al. A propensity-matched analysis between standard versus tapered oral vancomycin courses for the management of recurrent Clostridium difficile infection. Open Forum Infect Dis. 2017; 4(4):ofx235. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5729658/pdf/ofx235.pdf (accessed 2019 Mar 5).
Tomas ME, Mana TSC, Wilson BM et al. Tapering courses of oral vancomycin induce persistent disruption of the microbiota that provide colonization resistance to Clostridium difficile and vancomycin-resistant enterococci in mice. Antimicrob Agents Chemother. 2018; 62:e02237-17. https://aac.asm.org/content/62/5/e02237-17 (accessed 2019 Mar 5).
Sirbu BD, Soriano MM, Manzo C et al. Vancomycin taper and pulse regimen with careful follow-up for patients with recurrent Clostridium difficile infection. Clin Infect Dis. 2017; 65:1396-9.
Guery B, Menichetti F, Anttila VJ et al. Extended-pulsed fidaxomicin versus vancomycin for Clostridium difficile infection in patients 60 years and older (EXTEND): a randomised, controlled, open-label, phase 3b/4 trial. Lancet Infect Dis. 2018; 18:296-307.
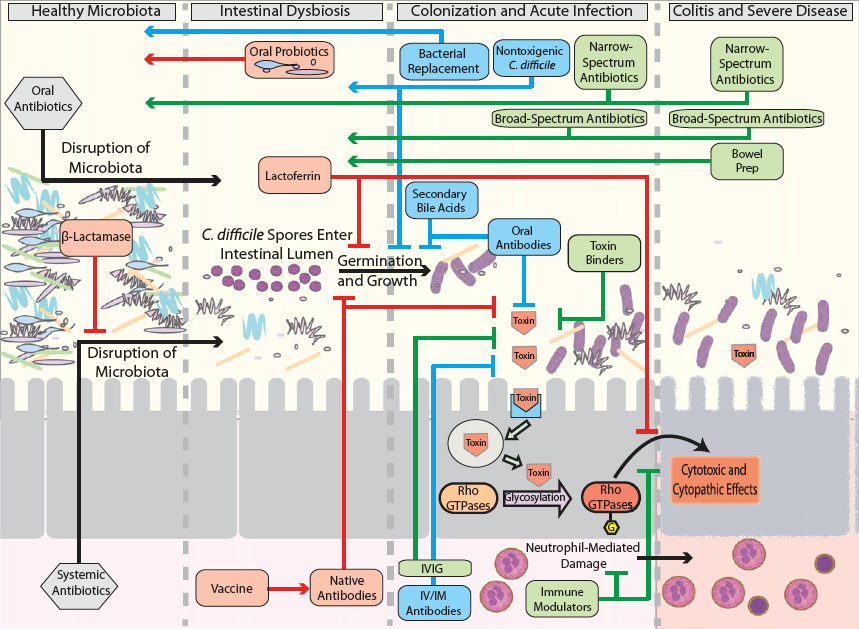
The high incidence and rate of recurrence of CDI have led to efforts to identify new modalities to prevent initial CDI episodes and prevent and treat recurrent CDI (Figure 2). New and emerging preventive strategies for CDI include probiotics to restore the normal microbiota, toxoid vaccines to elicit the production of antibodies that bind C. difficile toxins, and β-lactamase enzymes.
Ribaxamase is a novel, oral, recombinant β-lactamase enzyme that has been used in conjunction with intravenous (i.v.) β-lactam antibiotics for the prevention of CDI. Ribaxamase degrades excess β-lactam antibiotic secreted into the small intestine, thereby preventing disruption of the microbiota and CDI. Ribaxamase will not be useful for preventing CDI associated with non-β-lactam antibiotics because of its mechanism of action.
In phase 2a studies of 23 otherwise healthy patients who received ceftriaxone and had functioning ileostomies for ease of sampling of intestinal chyme, Kokai-Kun and colleagues demonstrated that ribaxamase was not absorbed after oral administration. Ceftriaxone levels in chyme were below the lower limit of quantification, and serum ceftriaxone levels were unaffected by ribaxamase. These effects were not affected by proton pump inhibitor use.
Figure 2. Emerging Therapeutic Targets for Management of CDIEmerging therapy therapeutic targets for management of CDI—prevention, primary treatment, and recurrence reduction.
Boxes indicate therapies, while arrows indicate the effect of the therapies. Black arrows indicate events and steps in the development of CDI. Starting with healthymicrobiota, antibiotic alterations lead to a susceptible state where C. difficile spores can enter
and germinate. This leads to colonization and infection. Toxin production can then trigger inflammation and cytotoxic/cytopathic effects on the mucosa, leading to colitis and severe disease. Red boxes and arrows indicate therapies aimed at preventing C. difficile infection. Green boxes and arrows indicate therapies aimed at treating primary CDI and reducing disease severity. Blue boxes and arrows indicate therapies aimed at reducing and treating recurrent CDI. IVIG, intravenous immunoglobulin.
Permission from Annals of the New York Academy of Sciences: Dieterle MG. Rao K, Young VB. Novel therapies and preventative strategies for primary and recurrent Clostridium difficile infections. 2019; 1435(1), Page 124.
These positive outcomes were shared with the Food and Drug Administration. The agency proposed efficacy and safety criteria that could be met in a single phase 3 clinical trial that is underway in patients receiving i.v. β-lactam antibiotics who are at high risk for CDI. Multiple β-lactam antibiotics will be evaluated. Data from such a trial may be sufficient for drug approval for the prevention of antibiotic-mediated CDI.
Oral narrow-spectrum, non-absorbable antibiotics (e.g., ridinilazole, cadazolid) that provide high intraluminal concentrations, limit systemic exposure, and do not disrupt the microbiota are in clinical trials for the primary treatment of CDI. Ridinilazole has potent anti-C. difficile activity and decreases inflammatory mediators (e.g., lactoferrin, calprotectin), although its mechanism of action is not completely clear. In a phase 2 randomized, double-blind, noninferiority study of 69 patients with CDI, ridinilazole (200 mg orally every 12 hours for 10 days) was superior to vancomycin (125 mg orally every 6 hours for 10 days) for providing a sustained clinical response (67% vs. 42%, respectively, p = 0.0004), which was defined as clinical cure at the end of treatment without recurrence within 30 days. The rate of recurrence was 14% in the ridinilazole group and 35% in the vancomycin group, representing a more than 50% reduction.
Nontoxigenic C. difficile spores have been used to prevent CDI recurrence by competing with disease-producing toxigenic strains. In a randomized, placebo-controlled study of 157 patients who had successfully completed vancomycin or metronidazole treatment for a first episode or first recurrence of CDI, a significantly lower rate of CDI recurrence at 6 weeks was demonstrated from the use of the nontoxigenic C. difficile M3 strain instead of placebo. Phase 2 clinical trials of this modality are in progress.
Fecal microbiota transplantation (FMT) is recommended in IDSA/SHEA treatment guidelines after appropriate antibiotic treatments have been used for at least two CDI recurrences. Research is needed to identify the target patient populations that stand to derive the greatest benefit from FMT; demonstrate its safety in immunocompromised patients (e.g., patients with IBD) and long-term safety in these and other patient populations; and identify the optimal route, preparation, and stool characteristics for FMT.
More Information
Kokai-Kun JF, Roberts T, Coughlin O et al. The oral β-lactamase SYN-004 (ribaxamase) degrades ceftriaxone excreted into the intestine in phase 2a clinical studies. Antimicrob Agents Chemother. 2017; 61(3):pii: e02197-16. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5328510/pdf/e02197-16.pdf (accessed 2019 Mar 5).
Vickers RJ, Tillotson GS, Nathan R et al. Efficacy and safety of ridinilazole compared with vancomycin for the treatment of Clostridium difficile infection: a phase 2, randomised, double-blind, active-controlled, non-inferiority study. Lancet Infect Dis. 2017; 17:735-44.
Gerding DN, Meyer T, Lee C et al. Administration of spores of nontoxigenic Clostridium difficile strain M3 for prevention of recurrent C. difficile infection: a randomized clinical trial. JAMA. 2015; 313:1719-27.
Faculty Biography
Kevin W. Garey, Pharm.D., M.S., FASHP, Activity Chair, Activity Chair
Professor and Chair
University of Houston College of Pharmacy
Houston, Texas
Kevin W. Garey, Pharm.D., M.S., FASHP, is Professor and Chair of the Department of Pharmacy Practice and Translational Research at the University of Houston College of Pharmacy in Houston, Texas. Dr. Garey is also Adjunct Professor at the University of Texas School of Public Health and Clinical Specialist and Researcher at Baylor St. Luke’s Medical Center in Houston.
Dr. Garey received a Bachelor of Science in Pharmacy from Dalhousie University in Halifax, Nova Scotia, Canada, a Doctor of Pharmacy from SUNY Buffalo in Buffalo, New York, and a Master of Science in Biometry from the University of Texas School of Public Health. His postdoctoral training includes a pharmacy practice residency at Bassett Healthcare, Cooperstown, New York, and infectious disease specialty residency and fellowship training at the University of Illinois at Chicago, Chicago, Illinois.
Dr. Garey is a member of the Infectious Diseases Society of American (IDSA) Standards and Practice Guidelines Committee and is a member of the IDSA-Society of Healthcare Epidemiology of America (SHEA) practice guidelines for C. difficile infection (CDI). He is an active member of the Society of Infectious Diseases Pharmacists (SIDP) and the American Society of Health-system Pharmacists (ASHP). He has been awarded several national awards including the ASHP Best Practices Award in Health-system Pharmacy Administration (2010), the ASHP Drug Therapy Research Award (2007), and the SIDP Impact Paper in Infectious Diseases Pharmacotherapy Research Award (2007, 2012). He received the University of Houston PLS leadership award in 2013. Dr. Garey's research, supported by the National Institute of Health, the Centers for Disease Control and Prevention, and the pharmaceutical industry, involves clinical and translational research in healthcare-associated infections including post-surgical infections, candidemia, and CDI. He has published over 200 peer-reviewed articles including identification that a delay in therapy for patients with candidemia impacts mortality and identification of a genetic risk for CDI.
Faculty Biography
Krishna Rao, M.D., M.S.
Assistant Professor
University of Michigan
Ann Arbor, Michigan
Krishna Rao, M.D., M.S., is Assistant Professor of internal medicine at Michigan Medicine at the University of Michigan in Ann Arbor, Michigan. He received his Doctor of Medicine degree from Rush University Medical Center in Chicago, Illinois and completed a pediatrics residency and an infectious diseases fellowship at the University of Michigan in Ann Arbor. He also received a Master of Science degree in Clinical Research Design and Statistical Analysis from the University of Michigan School Of Public Health.
Dr. Rao’s clinical, administrative, and research interests include the diagnosis and management of healthcare-associated infections, especially Clostridium difficile infection. His clinical work includes managing the University of Michigan Fecal Microbiota Transplantation (stool transplant) program for recurrent Clostridium difficile infection, a program that he co-founded. His primary research goal is to investigate how biochemical, microbiological, and clinical factors can help clinical decision-making in healthcare-associated infections, and he hopes to ultimately integrate these factors into robust risk-prediction algorithms for use by clinicians. He is currently funded by the National Institutes of Health (NIH) and the Centers for Disease Control and Prevention (CDC) on studies pertaining to C. difficile infection, the effect of antibiotics on the gut microbiota, and infections from Gram-negative bacteria, including multi-drug resistant organisms, such as Klebsiella pneumoniae.